Blood flow is the body’s earliest shared signal.
Why continuous blood-flow modeling reveals system-wide stress before symptoms, visits, or emergencies.
One signal. Many systems. Earlier understanding.
The unified carrier
Blood flow has one job: to deliver what the body needs and remove what it doesn't. Oxygen, nutrients, hormones, heat, waste, and signaling molecules all travel the same highway.
To do this, it must respond continuously to the demands of every major system—heart function, vascular tone, nervous regulation, kidney fluid balance, and metabolic state.
Blood flow isn’t just circulation—it’s the body reacting to itself.
The Gap
Why snapshots fail
Traditional vitals capture moments. But bodies change gradually. Deterioration shows up as drift, not sudden spikes.
By the time a single point is "out of range," the underlying issue has often been developing for weeks. We focus on the trajectory, not the event.
Health rarely fails suddenly. It drifts there.
Example
Anatomy of a lead-up
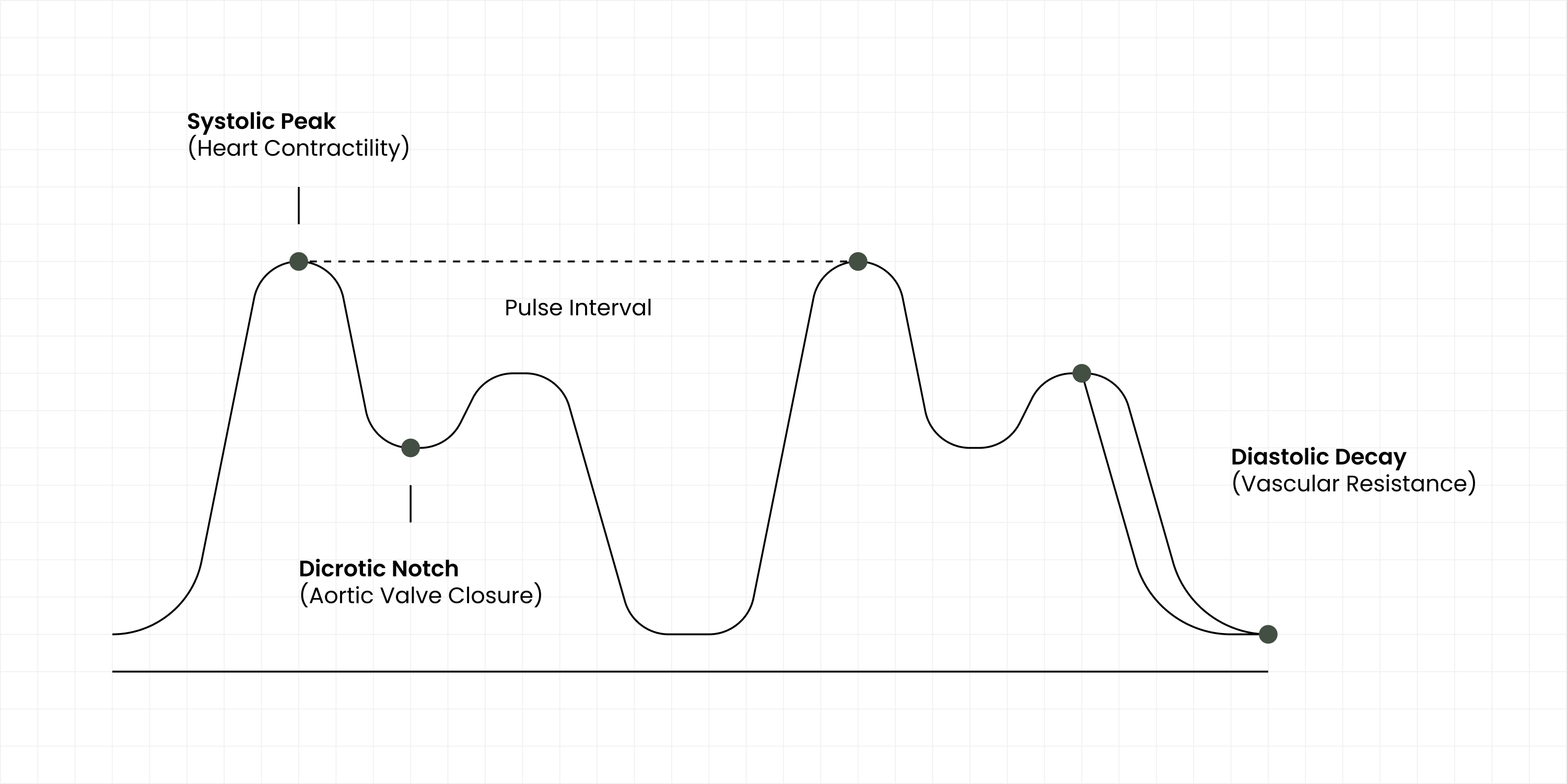
Consider the weeks before a cardiovascular event. You don't feel it, but the physics of your blood flow are changing to compensate.
Arteries narrow
Resistance increases, forcing pressure up.
Vessels stiffen
Waveforms become sharp and reflective.
Cardiac strain
Heart works harder, weakening forward flow.
Blood flow changes because the body is already compensating.
The foundation model
Our system builds a living baseline for every individual. It learns what "normal" looks like for you, so it can recognize meaningful change—not by crossing a generic threshold, but by deviating from your personal history.
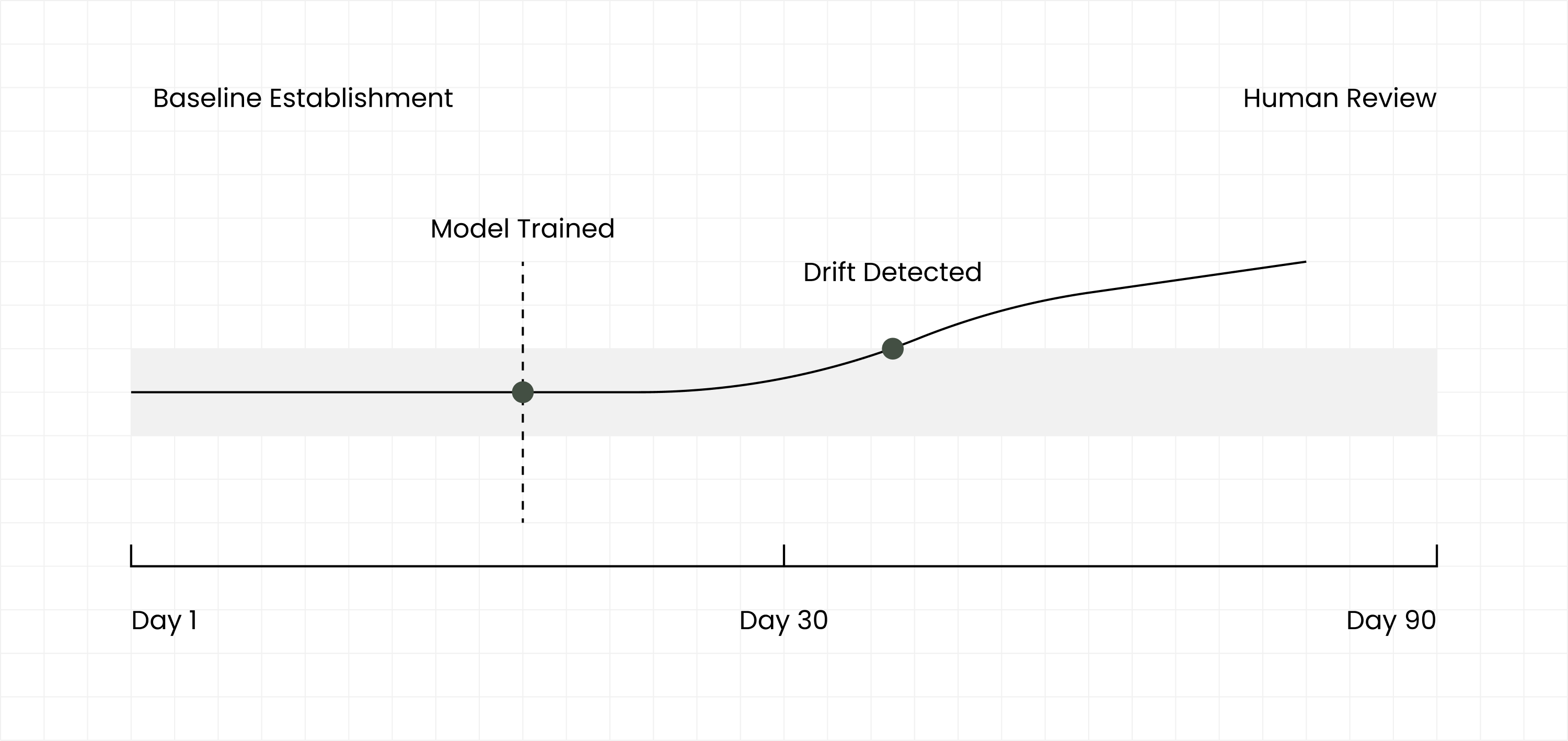
The model does not diagnose. It recognizes meaningful change.
"Technology detects patterns. Humans decide what they mean."
Human Interpretation
Context matters. Algorithms are excellent at detecting statistical drift, but they cannot know if you just ran for a bus or had a stressful phone call.
Our nurses act as stewards of the baseline. They interpret the change, filter out the noise, and coordinate with primary care. We only intervene when it matters.
Clinical Validation
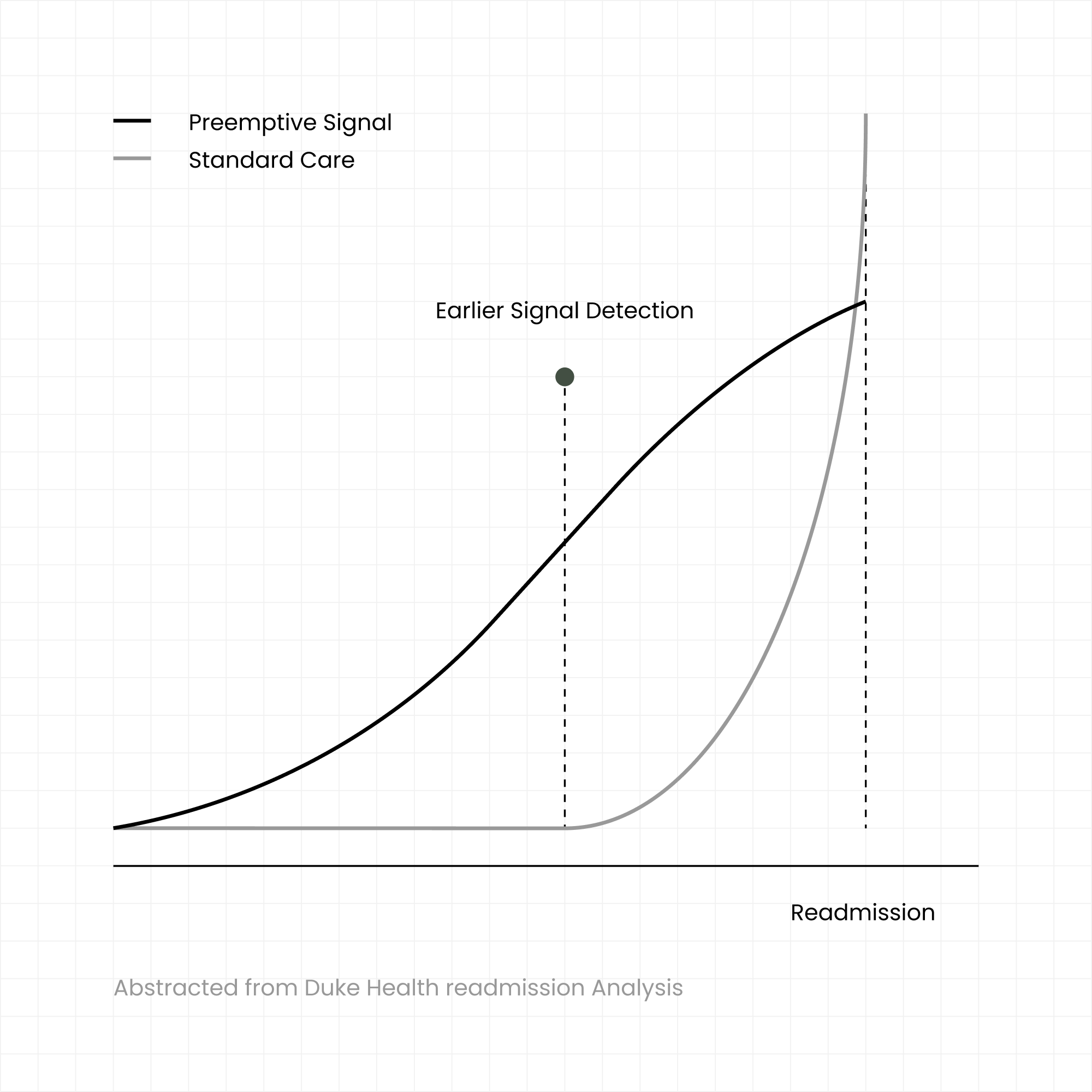
Validated in clinical practice
In collaboration with Duke Health, we evaluated Preemptive’s modeling approach in a real-world hospital readmission setting.
The study focused on identifying patients at risk of unplanned readmission. By analyzing continuous blood flow dynamics, the model demonstrated an ability to surface risk signals days before a readmission event occurred.
With an AUC of ~0.85, the model offered meaningful sensitivity with low false positives—providing a clear window for intervention that traditional clinical risk models often miss.
This study reflects how early physiological modeling can support earlier, calmer intervention when combined with human judgment.
What the model sees
Different conditions leave different early signatures in blood flow. We categorize these as physiological patterns, not diseases.
Fluid Overload
Changes in volume and pressure often preceding heart failure decompensation.
Vascular Resistance
Stiffening or narrowing vessels indicating rising hypertensive stress.
Inflammatory Stress
Subtle metabolic shifts that can signal developing infection or flare-ups.
Autonomic Instability
Imbalance in the nervous system regulation of heart rate and tone.
Timing Irregularity
Micro-variations in beat-to-beat intervals suggesting electrical issues.
Action before urgency
When a signal is caught early, the intervention is often simple. A medication adjustment. A hydration plan. A visit to primary care next week instead of the ER tonight.
Compounding value
The longer the model observes, the more precise it becomes. A longitudinal baseline is an asset that appreciates over time, offering greater protection the longer you stay within the system.
A foundation changes everything above it.
We don't replace clinicians. We strengthen them. By removing the surprise of emergencies, we return stability to healthcare.